Figure 1
Download original image
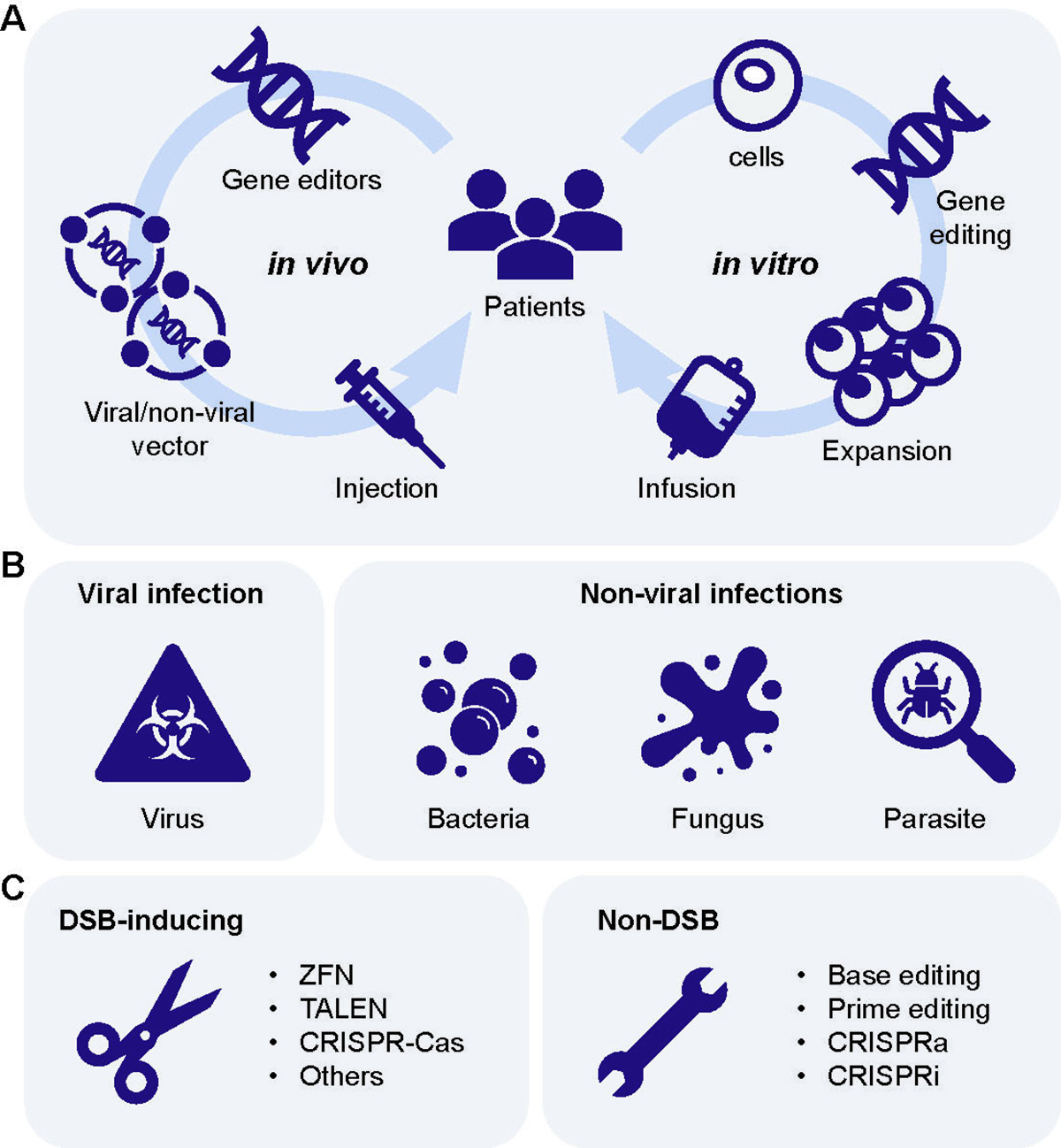
Gene therapy for infectious diseases. (A) Gene therapy is divided into two treatment strategies: in vivo and in vitro. The in vivo strategy (the left half) completes the treatment process by loading gene editing tools into viral or non-viral vectors and then injecting them into the body. The in vitro strategy (the right half) is to edit the patient’s primary cells, expand the edited cells, in vitro, and finally transfer them back to the patients. (B) Currently, gene therapy is aimed at two types of infectious diseases: viral (the primary pathogens are RNA or DNA viruses) and non-viral (the primary pathogens are pathogenic bacteria, fungi, and parasites) infection. (C) There are two types of gene editing tools: the DNA double-strand break (DSB)-inducing type and the non-DSB-inducing type. The former type acts like scissors. Under the guidance of gRNA, a DSB is introduced at a targeted location, where NHEJ or HDR is simultaneously induced to conduct the desired gene modification. These tools include ZFNs and TALEN, various CRISPR-Cas systems, and other nucleases (e.g., engineered ARCUS nuclease). The latter type, such as base editing, leader editing, gene activation (CRISPRa) and gene silencing (CRISPRi), completes the desired gene modification at targeted sites without DSBs. Such gene editing tools mainly derive from the CRISPR-Cas system, with fully inactivated dCas or partly inactivated nCas. Therefore, these gene editing tools are like wrenches, which repair or modify target sites, rather than destroying them.
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.